Listening as a tool to Tackle Stigma: Six practical strategies for individuals and organisations
Listening to patients and communities is central to high-quality care. But listening isn’t just a personal skill. It’s also a system design choice.
At an individual level, how we ask questions, respond to emotion and structure conversations shapes whether patients feel safe, believed and respected. At an organisational level, whether insights are captured, analysed and acted on determines whether listening leads to change.
Below are six evidence-based approaches. The first three focus on individual clinicians and healthcare workers. The second three focus on systems and services. What ones do you use?
Three ways individuals can listen better
Practice active listening
Active listening means being fully present and showing someone you’re genuinely trying to understand them. In healthcare, it means more than staying silent while someone speaks. It’s a deliberate practice of reflecting, clarifying and validating what you’ve heard.
As this month’s Tackling Stigma Champion, Gillian Love, puts it:
“Active listening is really important. That includes reflecting back what you’ve heard: ‘I heard you say this, is that what you meant?’ It includes neutral but validating statements like, ‘I can see this has really affected you. Those kinds of responses make people feel heard in a human way, not just a clinical one. Small tweaks in how we communicate can make a big difference.”
In practice, that might sound like:
“I want to make sure I’ve understood you correctly.”
“It sounds like this has really stayed with you.”
“Did I get that right?”
These small shifts reduce misinterpretation, signal respect, and give patients the chance to correct you. In stigma-sensitive contexts, that can be the difference between someone opening up or shutting down.
2. Invite narrative, not just information
Many healthcare interactions are structured around checklists, risk factors and diagnostic criteria. That information matters. But it doesn’t always capture what the experience actually means to the person living it.
Narrative approaches encourage clinicians and others working in healthcare to invite the patient’s story before narrowing the focus. Stories often surface concerns that structured histories miss.
“I think that considering patients’ stories is so essential to thorough, holistic medical care. When you look at a patient from a narrative standpoint, you take them in as a whole person. It prevents you from processing them mindlessly as another diagnosis, another problem to be treated … narrative medicine encourages reflection in a way that deals emotionally, as well as practically, with encounters in the medical field. I think developing this skill helps you to be a better doctor and person,” Australian medical student in the Guardian, discussing narrative medicine.
According to one research paper, exploratory questions and prompts include:
What is worrying you most?
What else was happening at that time?
How do you feel [or react] when ...?
And Questions and prompts inviting change:
How else might you explain …?
Are there any other possibilities?
What would happen if ...?
3. Follow the 70–30 rule
One practical way to improve listening is to simply change the ratio of who speaks. Often used in leadership, a 70–30 split is recommended. In healthcare, this would translate to the patient or family speaking for around 70% of the time, and the healthcare worker speaking for 30%.
Maybe that ratio isn’t quite right for healthcare (work out what is right for you), and the point isn’t to measure it with a stopwatch. It’s to resist the instinct to fill the space with explanations, advice or reassurance too early, or to not give patients the chance to think and explain clearly. When we dominate the conversation, important details often stay hidden.
You can shift the ratio by:
Asking one open question at a time and waiting
Avoiding interrupting in the first minute
Letting the patient finish before summarising
Listening takes time. But it can also save time by reducing misunderstandings later.
Three ways organisations can listen better
Individual listening matters, but organisational listening can have an even greater and far-reaching impact.
Use experience-based co-design and patient journey mapping
Experience-based co-design (EBCD), originally developed by Glenn Robert and Paul Bate, moves listening beyond simple feedback collection. It brings patients, carers and healthcare workers together to identify emotional “touchpoints” across the care journey and redesign services collaboratively.
We’ve previously profiled patient journey mapping as one way to do this. Providence Health Care in British Columbia, for example, used Indigenous-led journey mapping to surface truths — both good and confronting — and translate them into concrete change. Queensland Positive People took a similar approach, capturing lived experience visually and using a graphic illustrator to bring the journey to life. The visual format made patterns, gaps and emotional turning points impossible to ignore.
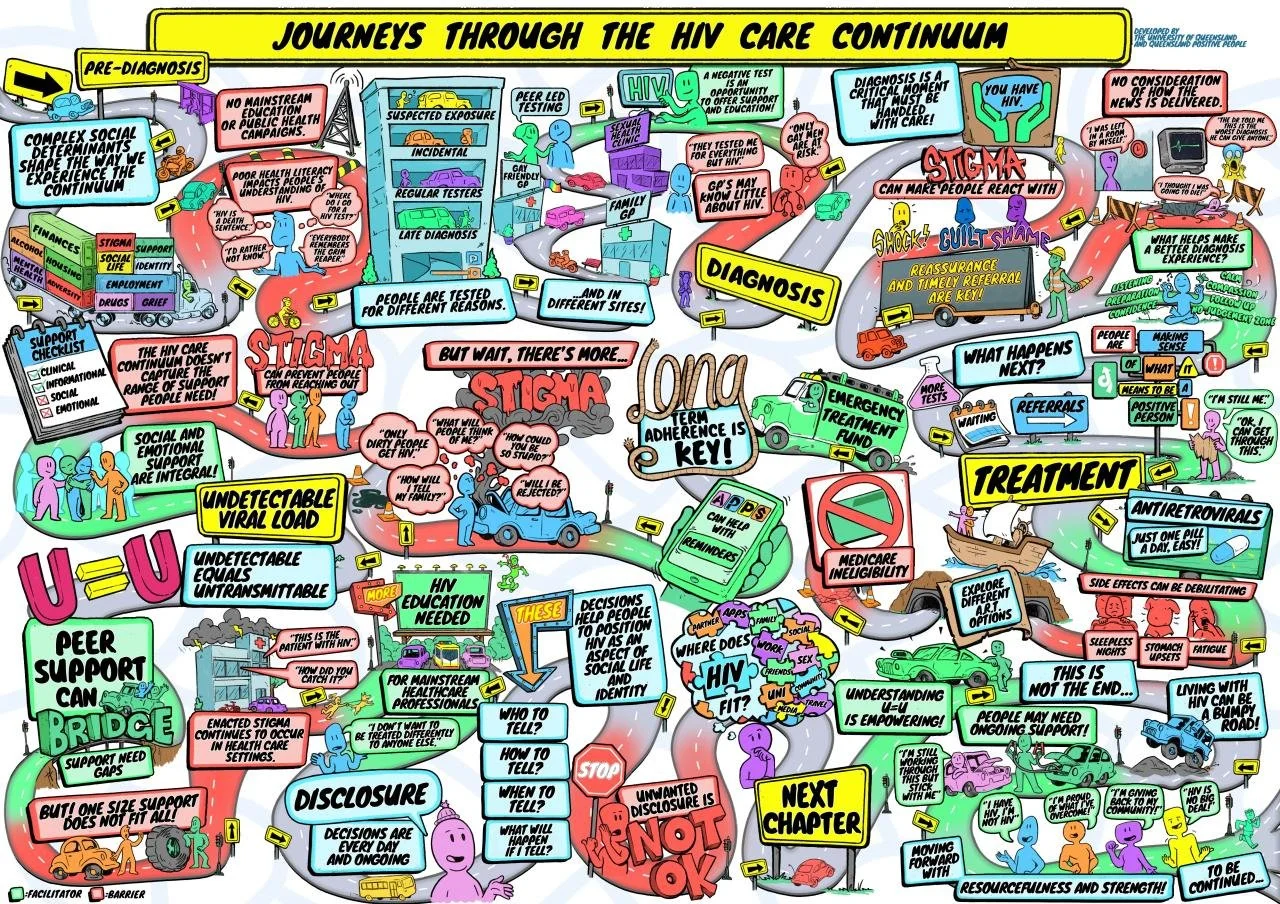
Image from Queensland Positive People, as shared with us on LinkedIn.
But co-design isn’t just about documenting experience well: it's about acting on it too.
In one project focused on hospital care for people with intellectual disability, cited in a synthesis of six EBCD projects across New South Wales, service users and carers identified recurring issues with communication, limited involvement in decisions, and poor transfer planning. These are common pressure points where people are spoken about rather than with.
Through co-design, the service developed practical structural responses: an online staff resource, lived-experience stories to strengthen understanding, and a personalised transfer folder to improve continuity of care. Listening was translated into tools that changed practice, not just perception.
2. Redesign complaints as a safe way to speak up
Complaints are often treated just as reputational risk. But they’re actually one of the clearest signals of where care has broken down.
In some countries like the UK, complaints are on the rise, but for people who experience stigma, formal complaints can feel unsafe. They might be worried about being labelled “difficult” or it impacting future care. If raising concerns feels risky, services are only hearing from those who feel confident enough to speak.
Organisations can change this by making complaints visibly safe and meaningful.
That might include:
Stating clearly that raising concerns will not affect future care
Offering anonymous or third-party reporting options
Publishing “You said, we did” summaries to show that feedback leads to change
When complaints are reframed as protected listening spaces rather than problems to manage, they can quickly become a powerful source of insight and help tackle stigma at its core.
3. Implement real-time or digital micro-feedback
Healthcare isn’t the only sector that relies on feedback. Retail and service industries show that feedback collected immediately after an interaction (such as the Net Promoter Score, which measures customer satisfaction) produces higher response rates. Short recall windows reduce memory bias and capture emotion while it’s still fresh, and could even lead to more specific, actionable insights than surveys conducted weeks or months later.
The same logic applies in healthcare.
Instead of relying solely on annual patient experience surveys, consider complementing them with real-time micro-feedback:
One question sent within 24 hours of an appointment via text or WhatsApp message
A short prompt such as “Did you feel heard today?” or “Would you return to this service and why?”
Open text fields, not just rating scales
When designed well, digital micro-feedback isn’t about replacing deeper qualitative work. It’s about strengthening it by capturing insight at the point it matters most, and also making patients feel heard.