Tackling Stigma Champion #6: Dr. Bruce Agins on quality improvement and the future of stigma reduction in HIV
Tackling Stigma Champion #6
To mark World AIDS Day, we spoke with Dr. Bruce Agins, creator of the Southeast Asia Stigma Reduction QI Learning Network (QIS+D), and Professor, Division of Infectious Disease Epidemiology Institute for Global Health Sciences, University of California San Francisco. Bruce has spent four decades at the forefront of HIV care, from the earliest days of the epidemic in the United States to his current work supporting governments across Southeast Asia to reduce stigma using data-driven, sustainable approaches.
Bruce’s central message is clear: stigma is not unbeatable. With the right tools — measurement, meaningful engagement with communities, local leadership, and a commitment to continuous improvement — health systems can build services where people feel respected, safe, and seen.
Bruce’s tips at a glance
Stigma is actionable. When you can measure it, you can change it
Some stigma drivers (fear, misinformation) are relatively easy to address; others (bias, beliefs) shift through meaningful interaction and self reflection
Community voices are critical in influencing leadership and shifting culture
Real progress happens locally: provinces, districts, and facilities shape people’s daily care experiences
Don’t separate HIV stigma from key population stigma: Intersectional stigmas shape people’s healthcare experiences.
Leadership and measurement are essential starting points for any stigma-reduction effort
Laura Nyblade’s validated measurement tools remain foundational to understanding healthcare-worker attitudes
Data must lead to action. Measurement alone isn’t enough
Quality improvement is one of the most powerful yet underused strategies for reducing stigma
Peer learning and shared indicators allow countries to make improvements together
Tell us a bit about yourself and how you became involved in stigma reduction
I entered HIV work at the very beginning of the epidemic in the United States and saw firsthand how stigma shaped those experiences. In the early days, many people developed Kaposi’s sarcoma, which was highly visible and amplified stigma.
Later, during my more than 25 years as Medical Director of AIDS Institute - New York State Department of Health, we built what I believe was the world’s first dedicated HIV quality improvement program. As services began using quality improvement tools like root-cause analysis, stigma repeatedly came up as a reason for poor retention or viral suppression, and people would say, “Yes, that’s true… but what can we do about it?”
In the 2000s, we began spreading this HIV quality improvement work globally through HIVQUAL and later HEALTHQUAL, supporting Ministries of Health globally to build their own HIV quality management programs. But a turning point for stigma reduction came in 2014, when I heard Dr. Laura Nyblade present her validated healthcare worker stigma survey. Suddenly, we had something measurable — a doorway into applying quality improvement to stigma.
Working closely with my colleague Dan Ikeda and many others such as Dr. Kriengkrai Srithanaviboonchai and Dr. Laura Nyblade, we then founded The Southeast Asia Stigma Reduction QI Learning Network (QIS+D), funded initially by PEPFAR.
Tell us more about The Southeast Asia Stigma Reduction QI Learning Network (QIS+D)
The QIS+D approach combines three things: measurement, improvement, and shared learning.
Participating facilities regularly measure stigma among healthcare workers using common indicators, alongside patient experience and treatment literacy.
They use this data to apply quality improvement methods such as mapping problems, testing small changes, and tailoring solutions to their context. We also promote organizational structures and processes to sustain these activities, hopefully integrated into their existing quality and HIV programs.
Countries then meet semi-annually to learn from each other, share what’s working, and plan how to scale and sustain the work.
To make this possible, we needed shared measures. So, from Laura Nyblade’s 51-item healthcare worker stigma scale, we used a modified Delphi process with country leadership to select eight priority measures across domains like:
fear of transmission
attitudes toward people living with HIV
knowledge gaps
institutional environment
We then added standard measures of patient experience, and health literacy which correlates via self-efficacy with reducing stigma.
Can you share some tangible examples of changes projects from the QS&ID network that reduced stigma?
Absolutely. Here are two below, and we have more in our ‘Spotlight’ section.
Thailand: Using quality improvement to address internalised stigma
One example I really love comes from Chiang Dao Hospital in Thailand. They use driver diagrams both to analyse causes of stigma and to define their interventions, and then they actually integrate the work into their hospital management system and assign responsibility so it becomes an organisation-wide effort.
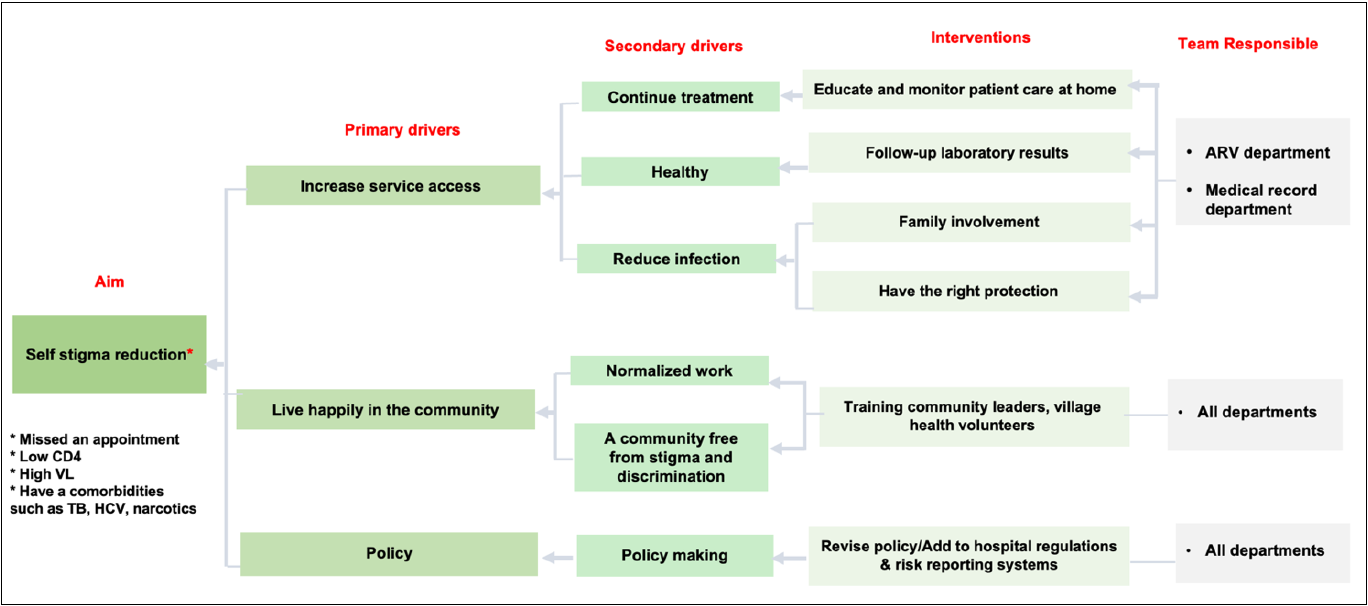
In this case the hospital chose to focus on internalised stigma, which is not a typical priority for healthcare organizations. Their driver diagram identified service-access issues, community issues, and policy issues as the main contributors, and then broke those down into secondary drivers that could be acted on.
The interventions included things like home education and patient follow-up, family involvement, infection-control precautions, partnering with the community, and addressing structural and policy barriers. It’s a comprehensive model, and the results were clear: improvements in stigma reduction were noted. The Thai Ministry of Health has standardised this approach so it can be used across hospitals in the country.
Malaysia: Project KASIH, a contact-strategy intervention
A very creative example comes from Malaysia, where a hospital implemented Project KASIH during COVID-19. They brought people from the HIV community into the hospital as volunteers — wheelchair navigators and guides, supporting all patients, not only people with HIV.
This worked in two directions. It created meaningful interaction between volunteers and healthcare staff, which reduced fear and concern among providers. And it empowered the volunteers, who became part of the care team.
The results were clear: stigma indicators dropped significantly in the second round of measurement. It’s a brilliant case of how communities and providers can come together to design strategies that work.
What does stigma look like across the countries you work with? Are there similarities or differences?
What we consistently see is that people are very satisfied with the care they receive in dedicated HIV clinics or community-based HIV programs. The challenges really show up when they have to intersect with the wider healthcare system — general hospitals, emergency rooms, maternity services, or other specialist clinics. That’s where stigma tends to surface, especially when care isn’t delivered in a dedicated HIV or community-based setting.
This matters because globally we’re moving toward universal healthcare with a primary-care model. Funding for dedicated services will diminish over time. Community clinics are adapting (many Key Population-led clinics are learning to bill insurance systems and sustain themselves) but we still need to redouble efforts to tackle stigma in the general healthcare system and in pre-service education. People who could benefit from HIV prevention are going to show up there, and that’s where the work needs to be.
Where should someone start if they want to reduce stigma in their own service?
Leadership and measurement. You need leaders who support the work, especially outside dedicated HIV settings. And you need data. Not just clinical data, but insight into healthcare-worker attitudes and patient experience. Laura Nyblade’s framework helps break this down into domains such as fear of transmission, attitudes, knowledge, and the institutional environment.
From there, you need a meaningful way to hear from patients. Satisfaction surveys alone won’t cut it. Services need qualitative feedback about people’s real experiences inside the facility and the barriers they face outside it. Pulling those pieces together takes time, commitment, and teamwork, but it’s the foundation for improvement.
What should countries be doing right now to advance stigma reduction?
I can’t underscore enough the importance of data-driven improvement. Measurement matters, but it’s only useful if it leads to action — the data have to be used to make changes. That’s where coaching, mentorship, education, and even public communication all play a role.

Thailand offers a strong example, taking a comprehensive, facility-wide approach that brings management, community members and healthcare workers together, and embeds stigma reduction into existing quality improvement (and Healthcare Accreditation) committees.
Health facilities don’t operate in isolation, and people who rely on them spend most of their lives outside their walls. That’s why the subnational level (provinces, districts, cities) is so important for aligning with national policy and sustaining the work.
Nakhon Ratchasima (Korat) in Thialand, does this subnational approach well and takes a "whole province approach", where everything really does come together.
The take-home message is that stigma is addressable. It’s actionable. And quality improvement is one of the most important yet often overlooked strategies we have to tackle. That’s why I value the Tackling Stigma initiative and the Stigma-Free Standard — quality improvement is central to your approach.
Can we tackle stigma?
Some drivers of stigma, like fear of infection or misinformation, are more straightforward to address through education and good infection-control practices. The harder issues are attitudes about sexual diversity, drug use, mental health, or strong religious convictions. But even these aren’t insurmountable.
We’ve seen examples globally, like these in Southeast Asia, where meaningful interaction with communities helps providers understand and overcome their biases. Across contexts, the message is the same: stigma is actionable, and people can change when they recognise their assumptions and engage directly with the communities they serve.